An Evaluation of Response to Treatment: The Lancashire and South Cumbria CFS/ME Services CBT Based Multi-Component Intervention
Lloyd M. Gemson[1], Mark P. Roy[2] and Gayle Brewer[3] from the Department of Psychology, University of Central Lancashire and David Riley[4] from The Lancashire and South Cumbria CFS/ME Services
Abstract
Chronic Fatigue Syndrome (CFS) is an illness which causes patients to experience disabling levels of fatigue, as well as chronic pain and cognitive abnormalities. Current evidence suggests that cognitive behavioural therapy (CBT) and graded exercise therapy (GET) can improve the symptoms of CFS. The aim of this audit project was to evaluate patients' response to a CBT-based multi-treatment used by The Lancashire and South Cumbria CFS/ME Services as an intervention. A repeated measures design was used to compare data from assessment, discharge, 12-month follow up and 24-month follow up. There were a total of 100 patients included in the audit project who had received treatment between 2006 and 2008. Repeated measures ANOVAs suggested significant improvements in patients' physical quality of life (P=0.001), psychological quality of life (P=0.008), fatigue levels (P<0.001) and depression levels (P=0.031). Improvements were maintained at the 12- and 24-month follow up. The overall findings of this audit demonstrate convincing evidence that the CBT-based multi-treatment used by The Lancashire and South Cumbria CFS/ME Services has a significant treatment effect, which appears to increase patients' physical and psychological quality of life, as well as to reduce levels of fatigue and depression.
Keywords: Chronic Fatigue Syndrome, Cognitive Behavioural Therapy, treatment, audit, intervention
Introduction
A report by The National Institute for Health and Clinical Excellence (NICE) recommended that patients suffering from Chronic Fatigue Syndrome (CFS) should be referred to a multidisciplinary team specialising in CFS (Turnbull et al., 2007). Patients should be presented with a tailored activity management treatment which draws on principles of cognitive behavioural therapy (CBT) and graded exercise therapy (GET) (Turnbull et al., 2007). In line with NICE recommendations, the Lancashire and South Cumbria CFS/ME Service developed a CBT-based multi-treatment with the goal of improving patients' physical and psychological quality of life. This is a preliminary evaluation of the Lancashire and South Cumbria CFS/ME Services' treatment programme based upon a retrospective audit of 100 patients who had completed treatment.
Chronic Fatigue Syndrome
CFS or Myalgic encephalomyelitis (ME) is a complicated and heterogeneous illness which is predominantly characterised by debilitating fatigue (Turnbull et al., 2007). Diagnosis occurs when a patient has experienced fatigue for at least six months which can not be explained by any other diagnosis (Surawy et al., 1995). In addition to fatigue, four or more of the following symptoms must also be present: impaired memory or concentration, sore throat, painful glands, muscle pain, multi-joint pain, new headaches, unrefreshing sleep and post-exertional malaise (Fukuda et al., 1994). In mild cases patients are able to walk for brief durations and may still be able to work part time (Cox, 1999); however, severe cases can result in patients being bed- and wheelchair-bound (Chambers et al., 2006).
The aetiology of CFS is ambiguous; however, premorbid stress increases the risk of developing the syndrome (Kato et al., 2009), and patients often report a viral infection prior to onset, although a single viral agent is unlikely (Afari and Buchwald, 2003). According to Fischler et al. (1997) there is a high prevelance of comorbid anxiety and depression within patients suffering from CFS, though it remains controversially unclear whether psychiatric illnesses contribute to the onset of CFS (Wood and Wessely, 1999). Therefore, CFS is likely to have multiple aetiological pathways (Afari and Buchwald, 2003).
The prognosis for recovery is varied and may be influenced by a number of factors, such as illness duration, the severity of comorbid psychiatric disorders, flexibility of the patient's illness beliefs and the degree of the patient's physical deconditioning (The Chief Medical Officer's Working Group Report on CFS/ME, 2002). Management techniques, such as CBT, can help patients to moderate the symptoms and manage the condition more effectively (Horton et al., 2010).
Management of CFS
Based on all available evidence, NICE has developed recommendations on how CFS should be managed in practice. It is recommended that patients are presented with a CBT and/or GET based treatment as they are the only evidence based treatments at present (Turnbull et al., 2007). CBT is a psychological treatment that draws upon the principles of cognitive therapy and behavioural therapy (Price et al., 2008). The cognitive aspects help patients to eliminate negative automatic thoughts in order to improve coping behaviour (Maes and Twisk, 2010), whilst the behavioural elements encourage gradual increases in activity to help the patient break through any limiting beliefs that can lead to physical deconditioning (Price et al., 2008). Studies show that CBT can successfully reduce fatigue levels in patients, as well as aid full recovery (Knoop Bleijenberg et al., 2007; Wiborg et al., 2010).
GET is an evidence-based approach that involves assessing a patient's physical ability and then gradually increasing it with supervised support to prevent symptom aggravation (Moss-Morris et al., 2005). In being prescribed gradual increases in aerobic exercise, patients experience improvements in their physical capability (Fulcher and White, 1997). Whites and Naish (2001) have shown that GET can double patients' exercise ability as well as their cardiovascular fitness.
Activity management is a person-centred approach that uses activity analyses and graded activity to improve physical ability and wellbeing (Turnbull et al., 2007). Friedberg (2002), shows that a treatment programme using graded activity resulted in a considerable increase in patient weight lifting intensity, walking time and a much better global clinical improvement rating.
Pacing is an energy management strategy which involves patients planning activities to incorporate periods of rest in order to prevent over-activity. Nijs et al. (2009) found that 3 weeks of a pace self-management treatment improved patients' daily functioning and fatigue levels without reducing their daily levels of activity.
NICE guidelines recommend that treatments such as activity management and pacing should be combined with CBT to offer a multi-component approach (Turnbull et al., 2007; Goudsmit, Ho-Yen and Dancey, 2009). This versatile approach aims to challenge physical deconditioning and the psychological impact of CFS, whilst emphasising the importance of pacing and activity management in order to prevent overexertion as well as emotional stress (Goudsmit et al., 2009; Maes and Twisk, 2010). CBT-based multi-treatments have been shown to reduce anxiety, fatigue and depression as well as improve self-efficacy (Ridsdale, Darbishire and Seed, 2004; Goudsmit et al., 2009; White et al., 2011).
Background of the Lancashire and South Cumbria CFS Services
The Lancashire and South Cumbria CFS Services at Preston was established in 2004 and is part of the Central Primary Care Trust. To date they have assessed and treated 1200 patients. Within their catchment area there are up to 6000 people with CFS, of whom 3000 may require support from health professionals.
Aim and Hypothesis of the Study
The purpose of this study was to audit the efficacy of the multi-component treatment offered to patients at The Lancashire and South Cumbria CFS Services, and to evaluate whether the effects were sustained at a one-year and two-year follow-up. It was predicted that there would be a significant response to treatment which would be demonstrated by improvements in patients' psychological and physiological quality of life, as well as improvements in patients' fatigue, depression and anxiety levels.
Method
Participants
A sample of 100 cases was drawn from the case notes archive of patients who had completed treatment between the years of 2006 and 2008, and who had records including assessment, discharge and 12-month follow up. During the process of data entry, the CFS services relocated and the author's documents were accidently destroyed. In order for the patients to be contacted with a 24-month review pack, patient files had to be accurately matched through variables in order to recover their data. Unfortunately, only 74 of the 100 patients could be confirmed through this process as some of the patients' files had been archived.
Materials
Self-Report Measures
Initial assessment form. This was filled in at assessment and gathered information about symptoms, sleep patterns, medication, perceived coping, significant stressful events and illnesses that the patient had experienced.
The World Health Organisation Quality of Life questionnaire short form (WHOQoL-BREF). This questionnaire is a cross-cultural self-report instrument that contains 26 items that score the patient's psychological, physiological, social and environmental quality of life on a five-point Likert scale (The WHOQoL Group,1998a).
The Hospital Anxiety and Depression Scale (HADS). This is a self-rating scale that evaluates secondary anxiety and depression in clinical settings. The scale is divided into two subscales; anxiety and depression. Each subscale uses 7 items and the total score range for each subscale can be between 0-21. Scores between 0-7 suggest healthy levels, 8-9 indicate a borderline clinical disorder, whilst 11 or above signifies a severe case of anxiety or depression (Zigmond and Snaith, 1983).
The Chalder Fatigue Scale. This is a 14-item scale that uses Likert scaling to measure physical and mental fatigue levels. The original scale contains 8 items for physical fatigue and 6 items for mental fatigue (Chalder et al., 1993). However, the scale used by The Lancashire and South Cumbria CFS/ME Services was reduced to 7 physical symptoms and 4 mental symptoms.
The 24-month review pack sent out to patients contained a contact letter explaining that The Lancashire and South Cumbria CFS/ME Services were performing an audit of their treatment programme, and that they would value patient feedback. The pack also contained the WHOQoL questionnaire, the Chalder Fatigue Scale and the HADS. For the analyses of the questionnaire scores, the Statistical Package for Social Sciences (SPSS) version 18 was used.
Procedure
Following approval by the Central Primary Care Trust and the University of Central Lancashire's ethics committee, information was collected from patients' files across three time points; assessment, discharge and 12-month follow up. Information was coded and entered into SPSS. All patient names were replaced with a number ID in order to protect anonymity. Once all patient data was entered, a subgroup were contacted with a 24-month review pack. Apart from the 24-month review pack no other contact was made with any of the patients regarding the study between the 12-month follow up and this time.
Results
Missing data
A total of 100 patient assessment questionnaire packs were entered into SPSS; however, there were problems with missing data, and many patients did not complete the full set of questionnaires. This was due to time factors, patients being too unwell to complete them, and patients leaving the treatment programme early. Table 1 shows the quantity of available data across the four time lines based on the original 100 patients.
| Measure | Assessment N |
Discharge N |
12 Months N |
24 Months N |
|---|---|---|---|---|
| WHOQoL Phys | 97 | 94 | 77 | 34 |
| WHOQoL Psyc | 100 | 94 | 77 | 34 |
| HADS Depress | 99 | 69 | 58 | 34 |
| HADS Anx | 99 | 69 | 58 | 34 |
| Chalder Fatigue | 91 | 92 | 59 | 33 |
Table 1: The quantity of patient data available for each measure across the four timelines
WHOQoL Physical
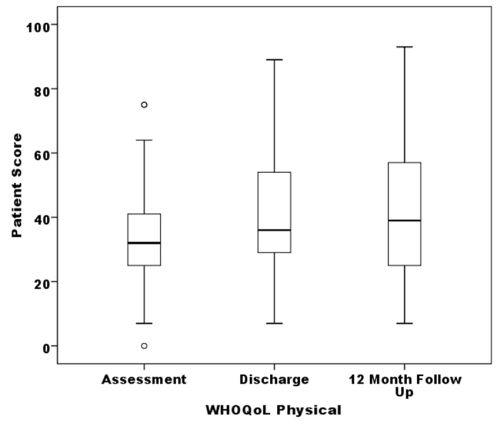
Figure 1: The WHOQoL physical scale scores across three timelines (N=71)

Figure 2: The WHOQoL physical scale scores between the 12- and 24-month follow-up (N=31)
The author undertook a series of repeated measures analyses of variance (ANOVA) in order to evaluate the data from patient self-report questionnaires at assessment, discharge, 12-month follow-up and at a 24-month follow-up. The results show that there were significant differences in the WHOQoL physical quality of life scale across three timelines, assessment, discharge and 12 months (F(1.89,132.23)=9.60, P=0.000, Eta²=0.12, Ob Power=0.97). Post hoc analyses revealed a significant mean difference between assessment and discharge (MD= 6.35, SE=1.77, P=0.001) as well as between assessment and 12 months (MD= 7.41, SE=2.03, P=0.001), but there was no significant mean difference between discharge and 12 months (see figure 1). When a subset of patients were followed up at 24 months, no significant difference was found between 12 and 24 months (F(1,30)=0.05, P=0.823, Eta²=0.00, Ob Power=0.06) although observed power was very low (see figure 2).
WHOQoL Psychological
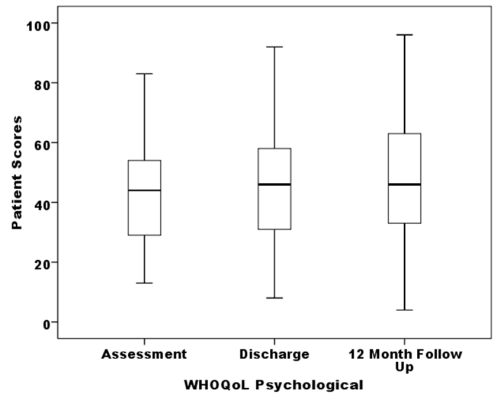
Figure 3: The WHOQoL psychological scale scores across the three timelines (N=72).

Figure 4: The WHOQoL psychological scores at the 12-month and 24-month follow-up (N=31).
A repeated measures ANOVA showed that there were significant differences in the patients' WHOQoL psychological quality of life scores (F(1.85,131.57)=6.24, P=0.003, Eta²=0.81, Ob Power=0.87). Post hoc comparisons demonstrated a significant increase in scores between assessment and discharge (MD=4.26, SE=1.57, P=0.008) as well as between assessment and 12 months (MD=5.36, SE=1.80, P=0.004), but there was no significant mean difference between discharge and 12 months (see figure 3). A subset of patients followed up at 24 months displayed no significant difference between 12 and 24 months (F(1,30)=0.27, P=0.611, Eta²=0.01, Ob Power=0.08), again the observed power was very low (see figure 4).
Chalder Fatigue

Figure 5: The Chalder Fatigue Scale scores across three timelines (N=52).

Figure 6: The Chalder Fatigue Scale scores at the 12 month and 24 month follow up (N=30).
A repeated measures ANOVA suggested a significant difference in patients' Chalder Fatigue scores across assessment, discharge and 12 months (F(1.99, 101.49)=20.41, P< 0.001, Eta²= 0.29, Ob Power=1.00). Further post hoc comparisons revealed a significant decrease in scores between assessment and discharge (MD= 6.04, SE=1.06, P<0.001) as well as between assessment and 12 months (MD= 5.75, SE=1.10, P<0.001), but there was no significant mean difference between discharge and 12 months (see figure 5). When a subset of patients were followed up at 24 months no significant difference was found between 12 and 24 months (F(1, 29)=3.56, P=0.069, Eta²=0.11, Ob Power=0.45) (see figure 6).
HAD Depression
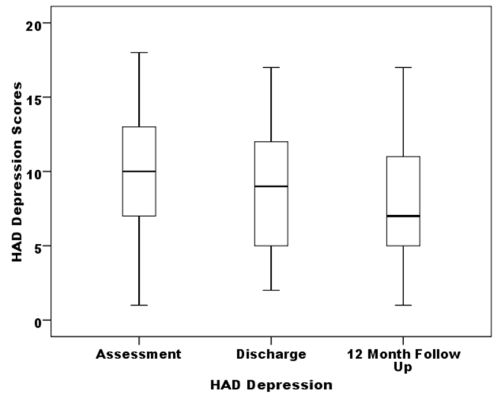
Figure 7: The HAD depression scores of patients across three time lines (N=54).

Figure 8: The HAD depression scores of patients at the 12 month and 24 month follow up (N=30).
A repeated measures ANOVA indicated that there was a significant difference between patients' HAD depression scores (F(1.79,94.81)=6.42, P=0.003, Eta²=0.11, Ob Power=0.87). Post hoc tests demonstrated that there was a significant mean difference in patients' HAD depression scores between assessment and discharge (MD=1.19, SE=0.53, P=0.031) as well as between assessment and 12 months (MD=1.70, SE=0.52, P=0.002), but there was no significant mean difference between discharge and 12 months (see figure 7). Analyses of a patient subset at 24 months demonstrated no significant difference in patients' depression levels between the 12- and 24-month follow-up (F(1,29)=0.17, P=0.680, Eta²=0.01, Ob Power=0.07), however, the ob power was very low (see figure 8).
HAD Anxiety
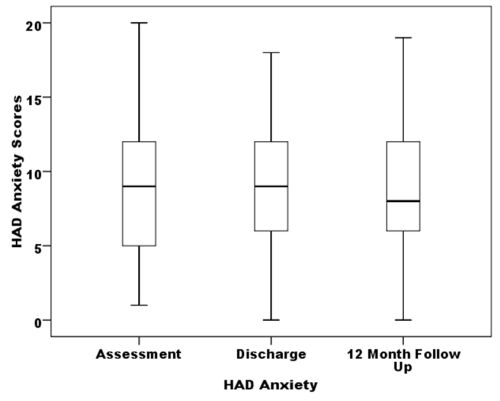
Figure 9: The HAD anxiety scores for patients across three time lines (N=54).

Figure 10: The HAD anxiety scores for patients at the 12-month and 24-month follow up (N=30).
A repeated measures ANOVA suggested that there was no significant difference for the HAD anxiety subscale (F(1.80, 95.18)=0.46, P=0.610, Eta²=0.01, Ob Power=0.12) (see figure 9). Further patient subgroup analyses at 24 months indicated that there was no significant difference for the HAD anxiety subscale between the 12- month and 24-month follow up (F(1,29)=1.03, P=0.319, Eta²=0.03, Ob Power=0.17) (see figure 10).
Discussion
The main aim of this study was to evaluate the effectiveness of a CBT-based multi-treatment implemented by The Lancashire and South Cumbria CFS/ME Services. It was predicted that there would be a significant treatment effect which would be demonstrated by improvements in patients' psychological and physiological quality of life, as well as improvements in patients' fatigue, depression and anxiety levels. Overall, the results of this study supported this hypothesis and demonstrated that patients had a significant response to the multi-component treatment. Furthermore, when measured at the 12-month and 24-month follow up the treatment effects had been maintained.
The results demonstrate that between assessment and discharge, patients experienced significant improvements in their (WHOQoL) physical quality of life, (WHOQoL) psychological quality of life, (Chalder Fatigue Scale) fatigue levels and (HAD) depression levels. When measured again at the 12-month follow up there was no significant change in these levels. This suggests that the CBT-based multi-treatment had the largest impact between assessment and discharge. Furthermore, these positive treatment effects were still maintained at the 12 month follow up. These results are consistent with the findings of other studies that have investigated CBT and activity based treatments (Friedberg 2002; Goudsmit et al., 2009; Nijs et al., 2009; Wiborg et al., 2010; White et al., 2011). However, it should be noted that this audit is evaluating a multi-component treatment that differs to previous studies in the way it is delivered and how the patients are assessed.
Unexpectedly, the analyses showed no significant change in patients' anxiety levels between assessment and discharge. This was a surprising finding as some studies investigating CBT-based treatments have demonstrated reductions in patient anxiety (Ridsdale et al.,2004; Goudsmit et al., 2009).
The results of the 24-month follow up displayed no significant changes in patient scores between the 12-month and 24-month follow up for (WHOQoL) physical quality of life, (WHOQoL) psychological quality of life, (Chalder Fatigue Scale) fatigue levels, coping ability, (HAD) depression, or (HAD) anxiety. This suggests that the positive treatment effects were sustained at the 24-month follow-up and that the treatment did not appear to have any effect on patient anxiety.
This study has a number of limitations that should be noted when interpreting the data. The first is the varying sample sizes and missing values that are illustrated in Table 1. It is possible that this could have affected the data, as patients who improved may not have returned for the 12-month follow-up, or taken part in the 24-month follow-up (as seen by the low observed power). In addition, missing data may also indicate that patients were too unwell to take part in the follow-ups. Due to the quantity of missing values, sample sizes were considerably reduced for various analyses. Finally, patients that took part in the follow-ups may have also been affected by other illnesses, or been exposed to other treatments that could have influenced the results.
The main strength of this study was the respectable sample size between assessment and discharge, which was representative of patients that attend The Lancashire and South Cumbria CFS/ME Services for treatment. A further strength of this audit is that it has completed a two year follow up which has demonstrated that the main treatment effects are sustained up to 24 months after patient discharge.
In conclusion, the findings of this audit are that the CBT based multi-treatment appears to have a positive effect by significantly improving patients physical quality of life, psychological quality of life, fatigue levels and depression levels. The main effects occur within treatment and are sustained at the 12-month and 24-month follow-up. Therefore there appears to be compelling evidence to suggest that the CBT based multi-Component intervention used by The Lancashire and South Cumbria CFS/ME Services is an effective treatment for patients suffering from CFS.
Acknowledgements
The authors would like to thank all the team at the Lancashire and South Cumbria CFS/ME Services and every patient involved in this audit.
List of Tables
Table 1: The quantity of patient data available for each measure across the four timelines
List of Illustrations
Figure 1: Boxplot showing The World Health Organisation Quality of Life questionnaire scores for patients' physical quality of life across assessment, discharge and 12-month follow-up
Figure 2: Boxplot showing The World Health Organisation Quality of Life questionnaire scores for patients' physical quality of life at the 12-month and 24-month follow-up
Figure 3: Boxplot showing The World Health Organisation Quality of Life questionnaire scores for patients' psychological quality of life across assessment, discharge and 12-month follow-up
Figure 4: Boxplot showing The World Health Organisation Quality of Life questionnaire scores for patients' psychological quality of life at the 12-month and 24-month follow-up
Figure 5: Boxplot illustrating the Chalder Fatigue Scale scores for patients across assessment, discharge, and 12 months
Figure 6: Boxplot illustrating the Chalder Fatigue Scale scores at the 12-month and 24-month follow-up.
Figure 7: Boxplot showing The Hospital Anxiety and Depression patient subscale scores for depression across assessment, discharge and 12 months
Figure 8: Boxplot showing The Hospital Anxiety and Depression patient subscale scores for depression at the 12-month and 24-month follow-up
Figure 9: Boxplot showing The Hospital Anxiety and Depression patient subscale scores for anxiety across assessment, discharge and 12 months
Figure 10: Boxplot showing The Hospital Anxiety and Depression patient subscale scores for anxiety at the 12-month and 24-month follow-up.
Notes
[1] Lloyd graduated from the University of Central Lancashire in July 2011 with a degree in Health Psychology and is currently a volunteer at The Lancashire and South Cumbria CFS/ME Services. Lloyd is returning to university in September 2011 to undertake an MSc in Health Psychology.
[2] Mark in 1994 spent 6 months as a postdoctoral research assistant in the Wellcome Research Unit, Department of Psychiatry, Oxford University with Professors Anke Ehlers & David Clarke. In 1994 he took up an appointment as Assistant Professor in the Department of Biobehavioral Health at The Pennsylvania State University. In 2000 Mark joined the Department of Psychology at The University of Central Lancashire where he is now a Senior Lecturer in Health & Physiological Psychology.
[3] Gayle's primary research interests focus on the areas of physical attractiveness and relationships. She has recently extended this research activity to investigate the health status of vulnerable groups including domestic violence victims and prisoners. Research findings have been reported in a range of National and International press. Gayle is currently a Senior Lecturer at The University of Central Lancashire.
[4] David joined the NHS in 1971 and qualified as a clinical psychologist in 1975. He has had many different roles including primary care, mental health, vocational rehab, psychosexual counselling, chronic pain, chronic illness and clinical psychology training. David also managed the Blackburn Clinical Psychology and Primary Care Counselling Service before retirement in 2005. David returned to part time work focusing on helping people cope rather than on management and is currently the Clinical Psychologist at The Lancashire and South Cumbria CFS/ME Services.
References
Afari, N. and D. Buchwald (2003), 'Chronic Fatigue Syndrome: A review', The American Journal of Psychiatry, 160 (2), 221-36
Chalder, T., G. Berelowitz, T. Pawlikowska, L. Watts, S. Wessely, D. Wright and E. P. Wallace (1993), 'Development Of A Fatigue Scale', Journal Of Psychosomatic Research, 37 (2), 147-53
Chambers, D., A. M. Bagnall and S. Hempel (2006), 'Interventions for the treatment, management and rehabilitation of patients with chronic fatigue syndrome/myalgic encephalomyelitis: an updated systematic review', Journal of The Royal Society of Medicine, 99 (10), 506-20
Cox, D.L. (1999), 'Chronic Fatigue Syndrome - An Occupational Therapy Programme', Occupational Therapy International, 6 (1), 52-64
Department of Health (2002), A Report of the CFS/ME working Group: report to the chief Medical Officer of an Independent Working Group, London: Department of Health
Fischler, B., R. Cluydts, V. De Gucht, L. Kaufman and K. De Meirleir (1997), 'Generalized anxiety disorder in chronic fatigue syndrome', Acta Psychiatrica Scandinavica, 95, 405-13
Friedberg, F. (2002), 'Does graded activity increase activity? A case study of chronic fatigue syndrome', Journal of Behaviour Therapy and Experimental Psychiatry, 33, 203-15
Fukuda, K., S. E. Straus, I. Hickie, M. C. Sharpe, J. G. Dobbins and A. Komaroff (1994), 'The chronic fatigue syndrome: A comprehensive approach to its definition and study', Annals of Internal Medicine, 121, 953–5 9
Fulcher, K. Y. and P. D. White (1997), 'Randomised controlled trial of graded exercise in patients with chronic fatigue syndrome', British Medical Journal, 314, 1647-52
Goudsmit, E.M., D. O. Ho-Yen and C.P. Dancey (2009), 'Learning to cope with chronic illness. Efficacy of a multi-component treatment for people with chronic fatigue syndrome', Patient Education And Counselling', 77 (2), 231-36
Horton, S. M. C., F. Poland, S. Kale, M. L. Drachler, J. C. Leite, M. A. McArthur, P. D. Campion, D. Pheby and L. Nacul (2010), 'Chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME) in adults: a qualitative study of perspectives from professional practice', BioMed Central Family Practice, 11 (89), 1-13
Kato, K., P. F. Sullivan, B. Evengard and N. Pederson (2006), 'Premorbid Predictors of Chronic Fatigue', Archives of General Psychiatry, 63, 1267-72
Knoop, H., G. Bleijenberg, M. F. M. Gielissen, J. W. M. van der Meer and P. D. White (2007), 'Is a Full Recovery Possible after Cognitive Behavioural Therapy for Chronic Fatigue Syndrome?', Psychotherapy and Psychomatics, 76, 171-76
Maes, M. and F. N. M. Twisk (2010), 'Correspondence Chronic fatigue syndrome: Harvey and Wessely's (bio)psychosocial model versus a bio(psychosocial) model based on inflammatory and oxidative and nitrosative stress pathways', BioMed Central Medicine, 8, 35-49
Moss-Morris, R., C. Sharon, R. Tobin and J. C. Baldi (2005), 'A randomized controlled graded exercise trial for chronic fatigue syndrome: outcomes and mechanisms of change', Journal of Health Psychology, 10, 245–5 9
Nijs, J., I.van Eupen, J. Vandecauter, E. Augustinus, G. Bleyen, G. Moorkens and M. Meeus (2009), 'Can pacing self-management alter physical behavior and symptom severity in chronic fatigue syndrome? A case series', Journal of Rehabilitation Research and Development, 46 (7), 985-96
Price, J. R., E. Mitchell, E. Tidy and V. Hunot (2008), 'Cognitive Behavioural Therapy For Chronic Fatigue Syndrome In Adults', Cochrane Database of Systematic Reviews, 3, 1-88
Ridsdale, L., L. Darbishire and P. T. Seed (2004), 'Is graded exercise better than cognitive behaviour therapy for fatigue? A UK randomized trial in primary care', Psychological Medicine, 34, 37-49
Surawy, C., A. Hackmann, K. Hawton and M. Sharpe (1995), 'Chronic Fatigue Syndrome: A cognitive Approach', Behaviour, Research and Therapy, 33 (5), 535-44
The WHOQOL Group (1998a), 'The World Health Organization Quality of Life assessment (WHOQOL): Development and general psychometric properties', Social Science and Medicine, 46, 1569–85
Turnbull N., E. J. Shaw, R. Baker, S. Dunsdon, N. Costin, G. Britton, S. Kuntze and R. Norman (2007), Chronic fatigue syndrome/myalgic encephalomyelitis (or encephalopathy): diagnosis and management of chronic fatigue syndrome/myalgic encephalomyelitis (or encephalopathy) in adults and children, London: Royal College of General Practitioners
White, P. D. and V. A. C. Naish (2001), 'Graded exercise therapy for chronic fatigue Syndrome: An audit', Physiotherapy, 87(6), 285-88
White, P. D., K. A. Goldsmith, A. L. Johnson, L. Potts, R. Walwyn, J. C. DeCesare, H. L. Baber, M. Burgess, L. V. Clark, D. L. Cox, J. Bavington, B. J. Angus, G. Murphy, M. Murphy, H. O'Dowd, D. Wilks, P. McCrone, T. Chalder and M. Sharpe (2011), 'Comparison, of adaptive, pacing therapy, graded exercise therapy, and specialist medical care for chronic fatigue syndrome (PACE): a randomised trial', Lancet, 377, 823-36
Wiborg J. F., H. Knoop, M. Stulemeijer, J. B. Prins and G. Bleijenberg (2010), 'How does cognitive behaviour therapy reduce fatigue in patients with chronic fatigue syndrome? The role of physical activity', Psychological Medicine, 5, 1-7
Wood, B. and S. Wessley (1999), 'Personality And Social Attitudes In Chronic Fatigue Syndrome', Journal of Psychosomatic Research, 47 (4), 385-97
Zigmond, A. S. and R. P. Snaith (1983), 'The Hospital Anxiety and Depression Scale', Acta Psychiatrica Scandinavica , 67, 361-70
To cite this paper please use the following details: Gemson, L. M., M. P. Roy, G. Brewer and D. Riley, (2011), 'An Evaluation of Response to Treatment: The Lanchashire and South Cumbria CFS/ME Services CBT Based Multi-Component Intervention', Reinvention: a Journal of Undergraduate Research, British Conference of Undergraduate Research 2011 Special Issue, http://www.warwick.ac.uk/go/reinventionjournal/archive/bcur2011specialissue/gemsonroybrewerriley. Date accessed [insert date]. If you cite this article or use it in any teaching or other related activities please let us know by e-mailing us at Reinventionjournal at warwick dot ac dot uk.